
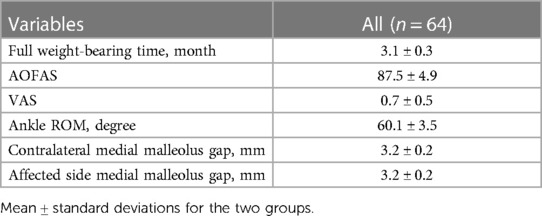
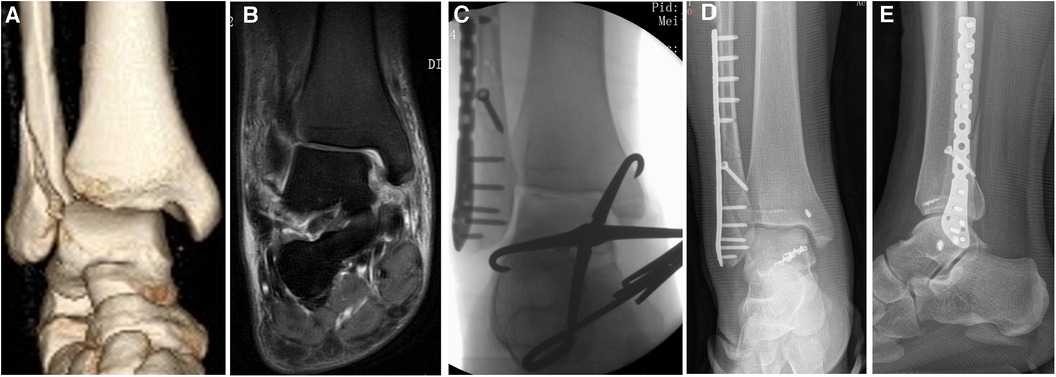
Deep deltoid ligament ruptures near the medial malleolar attachment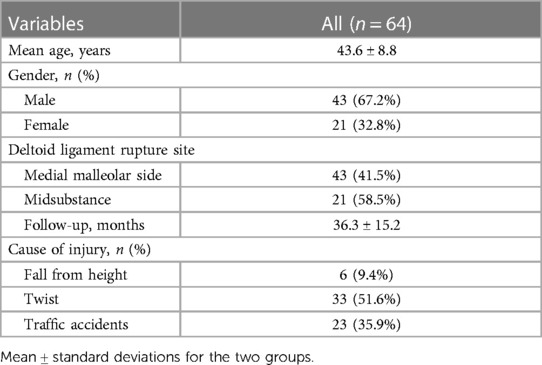 1Department of Orthopaedics, Lishui People's Hospital, The Sixth Affiliated Hospital of Wenzhou Medical University, The First Affiliated Hospital of Lishui University, Lishui, Zhejiang, China 2Department of Orthopaedics, Longquan People’s Hospital, Longquan, Zhejiang, China Purpose: Patients and methods: Results: Conclusion: The deltoid ligament origins at the medial malleolus and fans out to the medial side of the talus, calcaneus and navicular bones, including superficial and deep ligaments (1). It plays an important role in stabilizing the medial side of the ankle joint (2–4). The medial malleolar attachment is the most common site of deltoid ligament rupture (5, Suture anchor was usually inserted according to the rupture site of the deep deltoid ligament. If the deltoid ligament was ruptured near the medial malleolar attachment, the suture anchor was usually inserted into the medial malleolus. If the deltoid ligament was ruptured near the talar attachment, the suture anchor was usually inserted into the talus. For the case of midsubstance rupture of deltoid ligament, the deltoid ligament rupture was directly sutured. Previous studies showed that suture anchors into the talus had some unique advantages. The talar insertion area of the deltoid ligament is much broader than its origin in the medial malleolus (1), which is helpful to avoid the iatrogenic fracture of the medial malleolus when the suture anchor was inserted. Additionally, this procedure usually does not require a prolonged surgical incision and cause less trauma. To date, there is no study reporting suture anchor into the talus for treating deltoid ligament ruptures near the medial malleolar attachment or midsubstance rupture. Thus, the study first evaluates the clinical outcomes of suture anchor into the talus combined with transosseous suture in the medial malleolar for treating such deltoid ligament ruptures and promote its clinical application. Study population From Dec 2020 to Jun 2021, 64 patients with deltoid ligament ruptures in ankle fractures operated in our hospital were retrospectively analyzed. Deltoid ligament integrity was assessed by the presence of radiographic ankle dislocation and medial clear space wider than 4 mm, and intraoperative exploration. Our study was approved by the Ethics Committee of our hospital and was in accordance with the Helsinki Declaration. All patients gave informed consent and signed informed consent. Inclusion criteria of this study were (1) deltoid ligament full-layer ruptures in ankle fractures, which were determined by both preoperative MRI and intraoperative exploration; (2) deltoid ligament ruptures near the medial malleolar attachment or midsubstance rupture, which were determined by both preoperative MRI and intraoperative exploration; (3) those who were treated by suture anchor into the talus combined with transosseous suture in the medial malleolar. Exclusion criteria of this study were (1) Pathological fractures and open fractures (2) Those who cannot tolerate surgery (3) Follow-up data were incomplete and the follow-up time was less than 12 months. Surgical techniques The surgical procedure of deltoid ligament repair was as follows: (1) Vascular clamp was used to clear the synovial tissue outside the deltoid ligament, clearly reveal the broken end of the deltoid ligament, and identify the anterior and posterior edges of the ligament. (2) Two suture anchors were inserted at the talus, which were located at the anterior and posterior edges of the deep deltoid ligament. (3) A horizontal line with the articular surface of the lower tibia was drawn 1 cm above the tip of the medial anterior colliculus. At the intersection of the line with the middle and posterior 1/3 of the anterior colliculus and the anterior and middle 1/3 of the posterior colliculus, two holes were drilled with 2.0 mm Kirkler's needle at the talus attachment. Transosseous suture can provide stable repair. (4) We passed the tail line of the suture anchors through the two broken ends of the ligament (midsubstance rupture) or the whole process (medial malleolar attachment rupture), and then through the reserved holes in the medial malleolar. We tightened the tail line of the suture anchors and tied the knot after the talus—medial ankle relationship was restored with the reduction forceps. The superficial deltoid ligament can be repaired directly or by the suture anchor inserted at the anterior medial malleolar according to the deltoid ligament rupture site. The broken end of the ligament was investigated to confirm that the end-to-end involution was good at the broken end. (5) The excess part of the tail line of the suture anchors was used to suture the superficial layer of the deltoid ligament and the joint capsule. (6) After fractures were anatomically reduced and fixed, the ankle joint varsion external rotation stress test with x-ray was performed to observe the stability of the medial malleolus and the lower tibiofibular union. Static or dynamic fixation of the lower tibiofibular union was performed if necessary. Assessments All patients were followed up for at least 12 months. Clinical characteristics, cause of injury, and complications were recorded. The time to fracture healing and the time to full bear weight were documented during the follow-up. The clinical outcomes include the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score, visual analogue scale (VAS), and the active range of motion (ROM) of the ankle. In addition, medial malleolus gap was evaluated through x-ray. Statistical methods All statistical analyses were performed with SPSS 23.0 (IBM, Armonk, NY). Quantitative variables were presented in the form of mean ± standard deviation and categorical variables were shown in the form of frequency (%). A paired Patient characteristics A total of 64 patients were included in this study. Of the 64 patients, 43 were male (67.2%) and 21 were female (32.8%), with a mean age of 43.6 ± 8.8 years. According to deltoid ligament rupture site, 43 patients had injuries on the medial malleolar side, and 21 cases on the midsubstance. The causes of injury were falling from height (n = 6), twist (n = 33), and traffic accident (n = 23). All patients were followed up. The average postoperative follow-up duration was 36.3 ± 15.2 months (Table 1). Table 1 TABLE 1. Patient demographics. Clinical outcomes The mean full weight-bearing time was 3.1 ± 0.3 months. The mean AOFAS was 87.5 ± 4.9 and the average VAS was 0.7 ± 0.5. Additionally, the average ankle ROM of all patients was 60.1 ± 3.5 degrees. According to the postoperative radiological examination, there was no significance in medial malleolus gap between the contralateral side and affected side (p > 0.05) (Table 2). Table 2 TABLE 2. Clinical and radiographic outcomes. Wounds healed well in all patients. No neural damage, and deltoid re-rupture occurred. No infection and fracture nonunion were observed during the follow-up. Figure 1 Figure 1 FIGURE 1. A case of repairment for deep deltoid ligament rupture near the medial malleolar attachment by using suture anchors into the talus combined with transosseous suture in the medial malleolar. (A) Preoperative 3D reconstruction image showed increased medial malleolar space and ankle fracture. (B) Preoperative coronal MRI showed that the ruptured deltoid ligament. Combined with intraoperative exploration, the deltoid ligament was ruptured near the medial malleolar attachment. (C) Intraoperative anterior–posterior x-ray image showed the fixation of the talus—medial ankle relationship with reduction forceps. (D) Postoperative anterior–posterior x-ray image. The deep deltoid ligament was repaired by two suture anchors inserted at the talus. The superficial deltoid ligament was repaired by one suture anchor inserted at the medial malleolar. (E) Postoperative lateral x-ray image. Deltoid ligament injuries in ankle fractures are very common in clinical orthopaedics. Hintermann et al. (10) used arthroscopy to confirm that 40% of cases with ankle fractures were accompanied by deltoid ligament injuries, and the probability of complete deltoid ligament ruptures was 22.2%. However, there is no consensus on deltoid ligament repair in ankle fractures (4, Deltoid ligaments are usually repaired according to the different positions of ruptures. During the operation, we found that after the reduction of the medial malleolar space, the direct end-to-end suture of the midsubstance rupture was more difficult. Iatrogenic fracture of the medial ankle would occur when the anchor was treated at the medial ankle. Therefore, for deltoid ligament ruptures near the medial malleolar attachment or midsubstance rupture, we adopted the same method as that of deltoid ligament ruptures near the talar attachment. When the posterior and lateral structures of the ankle joint were not fixed and the medial malleolar space was not reduced, each suture anchor was inserted at the anterior and posterior edges of the deltoid ligament insertion point near the talus. After the reduction and fixation of the external and posterior ankle fractures were completed, the internal ankle space was restored with the reduction forceps, and then the tail lines of the suture anchors were tightened to tie the knot. At the same time, the anastomosis of the severed ligaments could be observed. This could avoid the difficulty of ligament suture in the narrow space. To prevent bone dissection during the transosseous suture at the medial malleolar, we covered the drills with the surrounding soft tissue, and then tied the knot of the tail line over the soft tissue. Chen et al. (18) found that deep deltoid ligament repair in treating supination-external rotation fracture displayed enhanced functional outcome, with an average AOFAS of 92.8 and a VAS of 0.79 at 12 months. For the ligament rupture at the endpoint of the medial malleolus, they placed two anchors at the posterior colliculus and intercollicular groove. However, this method usually requires a prolonged surgical incision to fully expose the deep deltoid ligament, with a corresponding increase in injury. Nacime et al. (19) repaired the deltoid ligament rupture arthroscopically and achieved an average AOFAS of 93.5 and a VAS of 0.75. They passed sutures using a suture passer, respecting the safe zone, on the area between the posterior tibial tendon and the saphenous vein (16–25 mm) (20). The average AOFAS and VAS in our study were 87.5 ± 4.9 and 0.7 ± 0.5, which was similar with their results. Overall, the results of our study suggest that suture anchor into the talus combined with transosseous suture in the medial malleolar for the treatment of deltoid ligament ruptures near the medial malleolar attachment or midsubstance rupture can achieve good clinical efficacy, which is worthy of clinical promotion and application. There are several limitations in this study. First, the retrospective nature of this study can generate bias. Second, this study was limited by the relatively small sample. Relevant clinical studies with larger sample sizes can be carried out in the future. Additionally, larger multi-center, prospective, randomized studies need to be carried out. Suture anchors into the talus combined with transosseous suture in the medial malleolar is a favorable treatment strategy for the deltoid ligament ruptures near the medial malleolar attachment or midsubstance rupture. The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. The studies involving humans were approved by Ethics Committee of Lishui People's Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. WL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft. MZ: Data curation, Formal Analysis, Investigation, Writing – review & editing. ZJ: Data curation, Formal Analysis, Investigation, Writing – review & editing. XM: Data curation, Formal Analysis, Investigation, Writing – review & editing. XZ: Data curation, Formal Analysis, Investigation, Writing – review & editing. FW: Conceptualization, Project administration, Resources, Supervision, Writing – review & editing. The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher. 1. Campbell KJ, Michalski MP, Wilson KJ, Goldsmith MT, Wijdicks CA, LaPrade RF, et al. The ligament anatomy of the deltoid complex of the ankle: a qualitative and quantitative anatomical study. PubMed Abstract 2. Loozen L, Veljkovic A, Younger A. Deltoid ligament injury and repair. PubMed Abstract 3. Stufkens SA, van den Bekerom MP, Knupp M, Hintermann B, van Dijk CN. The diagnosis and treatment of deltoid ligament lesions in supination-external rotation ankle fractures: a review. PubMed Abstract 4. Güvercin Y, Abdioğlu AA, Dizdar A, Yaylacı EU, Yaylacı M. Suture button fixation method used in the treatment of syndesmosis injury: a biomechanical analysis of the effect of the placement of the button on the distal tibiofibular joint in the mid-stance phase with finite elements method. Crossref Full Text 5. Crim J, Longenecker LG. MRI And surgical findings in deltoid ligament tears. PubMed Abstract 6. Woo SH, Bae SY, Chung HJ. Short-term results of a ruptured deltoid ligament repair during an acute ankle fracture fixation. PubMed Abstract 7. Park YH, Jang KS, Yeo ED, Choi GW, Kim HJ. Comparison of outcome of deltoid ligament repair according to location of suture anchors in rotational ankle fracture. PubMed Abstract 8. Wang J, Stride D, Horner NS, Petrisor B, Johal H, Khan M, et al. The role of deltoid ligament repair in ankle fractures with syndesmotic instability: a systematic review. PubMed Abstract 9. Guo W, Lin W, Chen W, Pan Y, Zhuang R. Comparison of deltoid ligament repair and non-repair in acute ankle fracture: a meta-analysis of comparative studies. PubMed Abstract 10. Hintermann B, Regazzoni P, Lampert C, Stutz G, Gächter A. Arthroscopic findings in acute fractures of the ankle. PubMed Abstract 11. Salameh M, Alhammoud A, Alkhatib N, Attia AK, Mekhaimar MM, D'Hooghe P, et al. Outcome of primary deltoid ligament repair in acute ankle fractures: a meta-analysis of comparative studies. PubMed Abstract 12. Güvercin Y, Yaylacı M. Biomechanical investigation of the effects of various treatment options on the talus in supination external rotation type 4 ankle injuries with ruptured deltoid ligament: finite element analysis. Crossref Full Text 13. Bastias GF, Filippi J. Acute deltoid ligament repair in ankle fractures. PubMed Abstract 14. Yang X, Zeng J, Yang W, Dela Rosa RD, Jiang Z. A meta-analysis of deltoid ligament on ankle joint fracture combining deltoid ligament injury. PubMed Abstract 15. Liao J, Zhang J, Ni W, Luo G. A retrospective study of deltoid ligament repair versus syndesmotic fixation in lateral malleolus fracture combined with both deltoid ligament injury and inferior tibiofibular syndesmotic disruption. PubMed Abstract 16. Hardy MA, Connors JC, Zulauf EE, Coyer MA. Acute deltoid ligament repair in ankle fractures: five-year follow-up. PubMed Abstract 17. Li H, Xue X, Tong J, Li H, Hua Y. Deltoid ligament (DL) repair produced better results than DL nonrepair for the treatment for rotational ankle instability. PubMed Abstract 18. Chen H, Yang D, Li Z, Niu J, Wang P, Li Q, et al. The importance of the deep deltoid ligament repair in treating supination-external rotation stage IV ankle fracture: a comparative retrospective cohort study. PubMed Abstract 19. Mansur NS B, Raduan FC, Lemos A, Baumfeld DS, Sanchez GT, do Prado MP, et al. Deltoid ligament arthroscopic repair in ankle fractures: case series. PubMed Abstract 20. Acevedo JI, Kreulen C, Cedeno AA, Baumfeld D, Nery C, Mangone PG. Technique for arthroscopic deltoid ligament repair with description of safe zones. PubMed Abstract
|

Shanghai Carefix Medical Instrument Co., Ltd.China
沪ICP备16042301号-1 (沪)-非经营性-2016-0122 沪食药监械生产许20101725号
