TYPES OF FRACTURE
Fractures are variable in appearance but for
practical reasons
they are divided into a few
well-defined
groups.
COMPLETE FRACTURES
The bone is
split
into two or more fragments. The fracture pattern on x-ray can help
predict
behaviour
after
reduction: in a
transverse fracture
the fragments
usually remain in place after reduction; if it is
oblique or spiral,
they tend to shorten and
re-displace
even if the bone is
splinted. In an
impacted fracture
the fragments are
jammed
tightly together and the fracture line is
indistinct. A
comminuted fracture
is one in which there are more than two fragments; because there is poor
interlocking
of the fracture surfaces, these are often unstable.
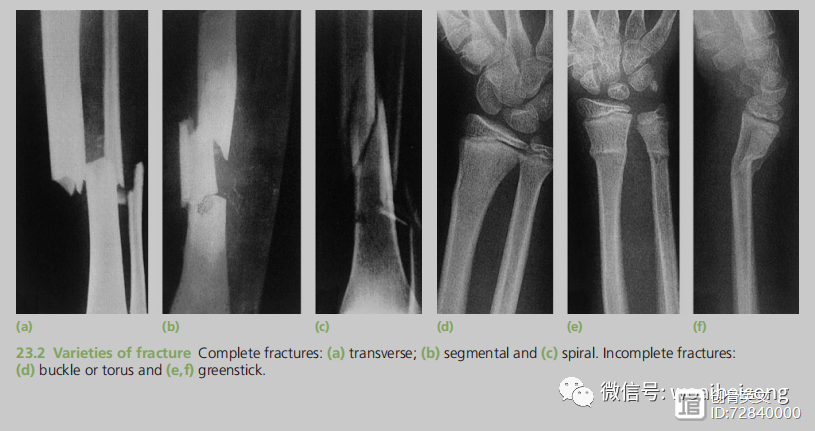
INCOMPLETE FRACTURES
Here the bone is incompletely divided and the
periosteum
remains in
continuity. In a
greenstick fracture
the bone is
buckled or bent
(like
snapping a green twig); this is seen in children, whose bones are more
springy
than those of adults. Children can also sustain injuries where the bone is
plastically deformed
(misshapen) without there being any crack visible on the x-ray. In contrast,
compression fractures
occur when cancellous bone is
crumpled. This happens in adults and typically where this type of bone structure is present, e.g. in the
vertebral bodies, calcaneum and tibial plateau.
CLASSIFICATION OF FRACTURES
Sorting fractures into those with similar features brings advantages: it allows any information about a fracture to be applied to others in the group (whether
this concerns treatment or prognosis) and it
facilitates
a common dialogue between
surgeons and others involved in the care of such injuries.
Traditional classifications, which often bear the
originator’s name, are
hampered
by being
applicable
to
that type of injury only; even then the term is often
inaccurately applied, famously in the case of Pott’s fracture, which is often applied to any fracture around
the ankle though that is not what Sir Percival Pott
implied when he described the injury in 1765.
A
universal, anatomically
based system facilitates communication and the sharing of data from a variety of countries and populations, thus contributing to advances in research and treatment. An
alphanumeric
classification developed by Müller and colleagues has now been
adapted and revised
(Muller et al., 1990; Marsh et al., 2007; Slongo and Audige 2007).
Whilst
it has yet to be
fully validated for reliability
and
reproducibility, it fulfils the objective of being
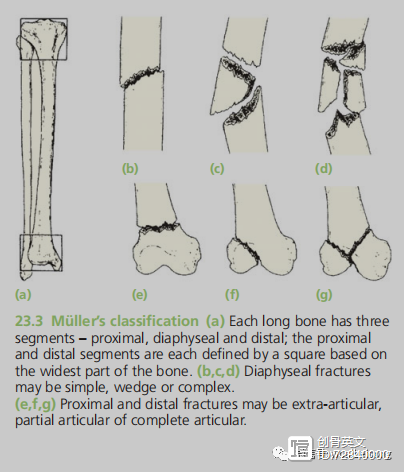
comprehensive. In this system, the first digit specifies the bone (1 = humerus, 2 = radius/ulna, 3 = femur, 4 = tibia/fibula) and the second the segment
(1 = proximal, 2 =
diaphyseal, 3 = distal, 4 =
malleolar). A letter
specifies
the fracture pattern (for the diaphysis: A = simple, B =
wedge, C = complex; for the
metaphysis: A = extra-articular, B =
partial
articular,
C = complete articular). Two further numbers specify the
detailed morphology
of the fracture (Fig. 23.3).
---from
《Apley’s System of Orthopaedics and Fractures》P687-688




